Need further support?
Continence Assessment form for a Child that has been toilet trained
The form below not only suggests which questions should be asked as part of a comprehensive continence assessment, but also explains why the questions should be asked and what the answers might mean. It signposts sources of further information and other useful tools.
The assessment form can therefore be used both to document a child’s bladder and bowel behaviour and as a teaching aid.
Use this form to assess a child who has been toilet trained. To assess a child who has not yet been toilet trained please use the Continence Assessment Form – Child who has not yet been toilet trained.
(**IMPORTANT** The word version must be used with the ERIC logo intact, OR if it is amended in any way after downloading, the ERIC logo needs to be removed and an acknowledgement of ERIC as the original author added saying 'Adapted from the ERIC original resource'.**)
| Bowels | Even if the presenting problem appears to be to do with the bladder, the starting point must be the bowels. This is because of the very close relationship between bladder and bowels; wetting can be entirely caused by constipation! |
| An assessment tool such as the Poo Diary should be used to document bowel activity, ideally for two weeks. | |
| Frequency of bowel actions:
____________ times a day/week |
The normal range is anything from three times a day to three times a week. However, most children poo every day. Children should be encouraged to poo at least every other day.
If child is pooing more frequently consider:
Is this constipation and/or overflow? See Advice for Children with Constipation for explanation. |
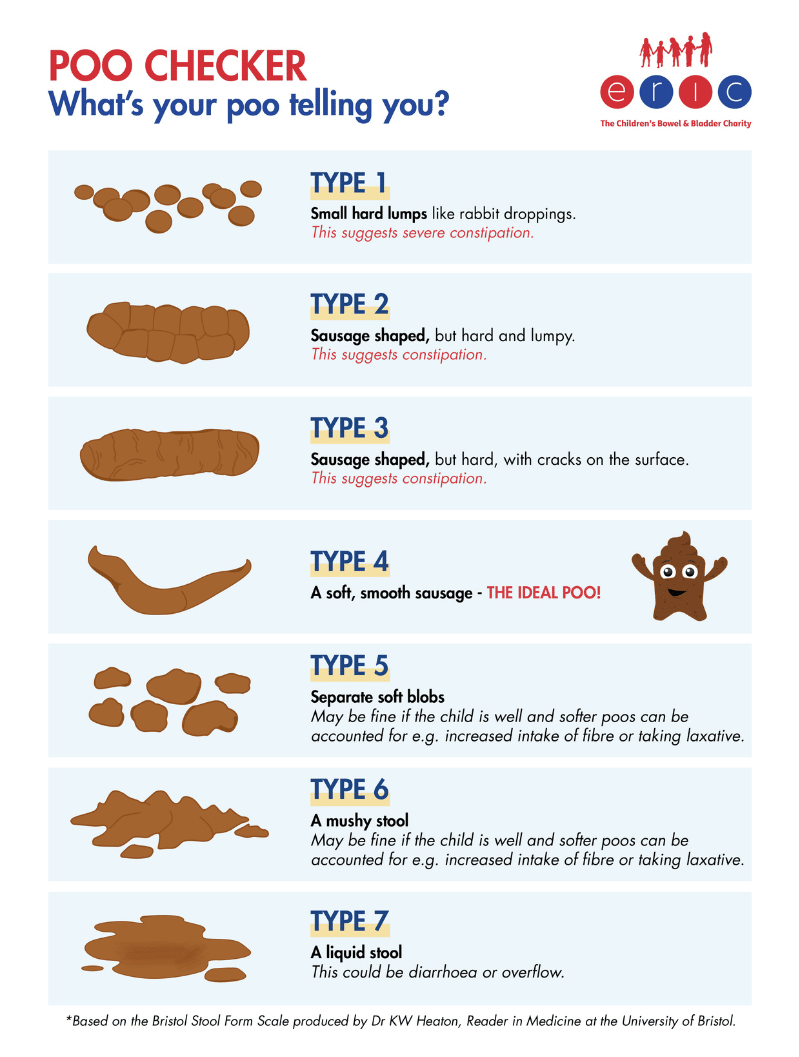
| Stool Type
1 2 3 4 5 6 7 |
Types 1-3 all suggest constipation in a child, with Type 1 being the most severe. Type 4 is the ideal poo! Types 5 & 6 may be fine if the child is well and softer stools can be accounted for (e.g. increased intake of fibre, taking laxatives). Type 7 could be diarrhoea or overflow. If child has persistent loose stools consider:
Is this overflow caused by constipation? See Advice for Children with Constipation for explanation. |
| Any soiling?
Yes / No If yes: Amount? Stain in pants or on pad / modest amount / full bowel action Several times a day / daily / less frequently |
If the child is soiling always suspect constipation – remember almost all childhood soiling is caused by functional constipation! |
| What protection does the child wear?
Pants / pad in pants / nappy / pull-up |
Consider if child is eligible for products from Continence Service. See Flowchart - Child with Additional Needs.
NB Additional needs can include organic underlying bladder/bowel conditions such as neuropathic bladder/bowels, ano-rectal anomalies, cloacal anomalies and significant learning disabilities. |
| Does the child use the potty / toilet / neither?
Is there a regular toileting programme in place? Yes / No |
|
| Does the child pass LARGE stools / large quantity of stool all at once?
Yes / No |
In order to pass a large amount of stool at once, the stool must have accumulated over a period of time. This represents constipation. The accumulated stool will stretch the rectum; if this is allowed to persist there will be a loss of rectal tone which will diminish the sensation of the need to poo. |
| Any abdominal pain and/or pain on defaecation?
Yes / No |
This could be caused by constipation. |
| Any abdominal distension?
Yes / No |
This could be caused by constipation. Note, the presence of gross abdominal distension represents a red flag finding (NICE Guidelines). |
| Any anorexia / nausea / vomiting / faltering growth?
Yes / No |
This could be caused by constipation. Note, the presence of faltering growth represents a red flag finding (NICE Guidelines). |
| Any other associated behaviour – straining / stool withholding / toilet avoidance / passing stools at night?
Yes / No |
This could be caused by constipation. |
| The child does not have to display all these symptoms to be diagnosed with constipation. See NICE Guideline CG99 – Constipation in children and young people - two or more findings indicate constipation. | |
| If constipation is indicated follow Flowchart for Constipation. | |
| Has child been seen by GP/Paediatrician for physical examination to rule out underlying organic cause – ‘red flags’?
Yes / No / Referred |
See NICE Guideline CG99 – Constipation in children and young people
Remember the child may have e.g. a very subtle spinal anomaly – constipation may be the only presenting symptom. The physical examination should not be omitted. |
| Daytime Bladders | Before beginning to assess daytime bladder symptoms, ensure the child has had a bowel assessment. This is because of the very close relationship between bladder and bowels; wetting can be entirely caused by constipation! |
| Frequency of voids:
_______________ times a day |
The normal range is considered to be 4–7 voids per day. Voiding frequency should be assessed in conjunction with an assessment of fluid intake – infrequent voids can of course be caused by an inadequate fluid intake, and vice versa! An assessment tool such as the Intake/Output Chart should therefore be used. A minimum of 48 hours should be recorded. |
| Urinary urgency
Yes / No |
International Children's Continence Society (ICCS) definition: "The sudden and unexpected, immediate and compelling or urgent need to pass urine." |
| Volume of voids:
Maximum voided volume ____________mls Expected bladder volume ____________mls |
Calculate the child’s expected bladder capacity using the formula (Age + 1) x 30 mls (for children aged 4-12 years).
How does their functional bladder capacity (volume voided) compare with their expected bladder capacity? Frequent small voids +/- urgency could be caused by:
Infrequent voids could be caused by:
If large volume could be caused by:
|
| Voiding behaviour:
Any hesitancy? Yes / No Any straining to initiate void? Yes / No Is stream weak/interrupted? Yes / No |
Any of these voiding behaviours could suggest Dysfunctional voiding. A weak stream could also be indicative of bladder outflow obstruction and should be investigated. |
| History of Urinary Tract Infection (UTI)?
Yes / No
Number of UTIs in the last year _________
Current UTI suspected? Yes / No
Urinalysis performed? Yes / No Result _______________________________
Specimen sent? Yes / No Result _______________________________ |
Symptoms may include:
Remember, children may not display all these symptoms. Check for asymptomatic bacteriuria if the child is well but has frequency / urgency / wetting. |
| If UTI confirmed see NICE Guideline CG54 – Urinary Tract Infections in under 16s | |
| Any daytime wetting?
Yes / No If yes: Amount? Damp pants / wet through to outer clothes / puddle Several times a day / daily / less frequently When do the problems primarily occur? Prior to voiding / after voiding / associated with laughing / randomly |
If wetting occurs prior to voiding:
If wetting occurs after voiding:
If wetting only associated with laughing, suspect Giggle Incontinence. Stress incontinence, i.e. wetting ONLY associated with raised intra-abdominal pressure (e.g. coughing, trampolining) occurs rarely in childhood. |
| What protection does the child wear?
Pants / pad in pads / nappy / pull-up |
Consider if child is eligible for products from Continence Service. See Flowchart - Child with Additional Needs.
NB Additional needs can include organic underlying bladder/bowel conditions such as neuropathic bladder/bowels, ano-rectal anomalies, cloacal anomalies and significant learning disabilities. |
| What are the child’s usual drinks?
_____________________________________ _____________________________________ |
Caffeine can cause bladder disturbance and should always be avoided.
Blackcurrant / orange / artificial colourings / flavourings / sweeteners / carbonated drinks are all bladder irritants for some people – so should be trialled to assess effect on individual child. |
| How many drinks does the child have every day? _____________________
Are drinks evenly spread throughout the day? Yes / No Average daily fluid intake? __________mls |
We all need to have at least 6-8 cups of water-based fluid every day, spread evenly over the day. The cup size should be appropriate to the child's size, e.g. about 200mls for a 7 year old, 250mls for an 11 year old. If fluid intake is inappropriate in type and/or quantity - correct, then re-assess bladder.
See Advice for Children with Daytime Bladder Problems for more information. |
| If daytime bladder problems are indicated follow Flowchart for Daytime Bladders. | |
| Has child been seen by GP/Paediatrician for physical examination to rule out underlying organic cause?
Yes / No / Referred |
Remember the child may have e.g. a very subtle spinal/urological anomaly – daytime bladder problems may be the only presenting symptom. The physical examination should not be omitted. |
| Night Time Bladders | Before beginning to assess night time bladder symptoms, ensure the child has had a bowel assessment. This is because of the very close relationship between bladder and bowels; wetting can be entirely caused by constipation!
Ensure that the daytime bladder is assessed and any symptoms treated before considering specific treatment for night time wetting. |
| Is the child occasionally or regularly wet at night?
Yes / No If yes – continue assessment below. If no – does the child get up to void during the night: Never / infrequent (less than 4 times a week) / frequent (4 or more times a week) / once a night / more than once a night. |
If the child wakes to void more than once a night check if caused by drinking close to bedtime/during the night.
If not, the child should be assessed to establish cause. Disturbed sleep can affect the child’s ability to concentrate at school. |
| Is the wetting:
Primary – the child has never been dry at night for a 6 month period? Secondary – the child has been dry at night for at least 6 months prior to this episode? |
Night time wetting may be associated with a systemic cause or trigger or comorbidities, e.g. UTI, constipation, Diabetes mellitus, psychosocial situation, neurological cause. |
| Does the child wake after wetting?
Yes / No |
Determining the exact nature of the night time wetting will help to determine primary cause and subsequently the optimum treatment. See Advice for Children with Night Time Wetting for explanation. Use Night Time Diary to record information.
Factors suggesting poor arousability:
-> consider alarm as first line treatment. Factors suggesting low Vasopressin:
-> consider desmopressin as first line treatment. Factors suggesting small functional bladder capacity (which may be due to overactive bladder):
-> ensure no constipation / optimal fluid intake / consider anticholinergic. NB Wetting may be caused by more than one reason. Combination treatment may be required. |
| Does the child wet once a night / more than once a night? | |
| Volume of wetting:
Just night wear / wet patch the size of a dinner plate / wet patch covering most of the middle of the bed / most of the bed wet, including pillow and duvet |
|
| Time of wetting:
Soon after going to bed / later in the night |
|
| Size of morning void:
Unable to void / small / medium / large |
|
| Colour of morning void:
Dilute / concentrated |
|
| Time of last drink
________ What time does the child go to bed? ________ Does the child void before going to bed? Yes / No Does the child void before going to sleep? Yes / No What time does the child go to sleep? ________ |
If there is a long interval between bed and sleep times check if child is getting up for ‘last minute wee’ – and if not, promote. Ask if child watches TV/plays computer games in bed – can disturb sleep patterns. |
| Does the child share a bedroom?
Yes / No Single bed / cabin / bunk – top/bottom |
Finding out about the sleeping arrangements will help rule out contributory factors and help to advise on treatment suitability. |
| Will the child go to the toilet if they wake?
Yes / No Any concerns? |
Consider:
Is the child afraid of the dark? If so, do they have a night light? Have they got a potty/bucket/bottle in their room? |
| See NICE Guideline CG111 – Bedwetting in under 19s | |
| If night time wetting is indicated follow Flowchart for Night Time Wetting. | |
This assessment complies with these national and international standard documents:
- NICE Guideline CG99 – Constipation in children and young people
- NICE Guideline CG111 – Bedwetting in under 19s
- International Children's Continence Society (ICCS) Terminology, Standardisation document, Assessment of daytime wetting (available through membership of the ICCS website)
Upcoming dates
Share this page